

Dr. Schreiber of San Augustine giving a typhoid inoculation at a rural school, San Augustine County, Texas, in April 1943, and an 1802 cartoon parody of the early controversy surrounding Edward Jenner’s vaccination theory, showing using his cowpox-derived smallpox vaccine causing cattle to emerge from patients. Images are in the public domain.
Children & the Coronavirus Vaccine
Abstract
The SARS-CoV-2 pandemic over the last year and a half resulted in swift vaccine development to thwart the virus. mRNA technology of which most were unaware produced the fastest vaccine rollout in history. Early on, health authorities focused on seniors who suffered the most. As we saw the rollout start there, health authorities began to promote the vaccine for younger and younger individuals with some advocating administration to children down to six months.
Are SARS-CoV-2 vaccines safe to give to children under 18? Should we be giving these vaccines to this age group at all? What does the data say?
In order to answer these questions, we must understand how the mRNA vaccine technology came about historically. A vaccine is not just one thing, but a carefully crafted biochemical response to the modus operandi of each infectious agent. This paper attempts to show the scope of the issues historically.
We will examine what the data says about SARS-CoV-2 pandemic. We think it shows that mRNA technology is good technology. However, questions exist about the lack of data-driven administration recommendations, as well as concern about the bureaucratic moves in those recommendations which appear to be politically rather than medically motivated. The Emergency Use Authorization by the FDA and others without quoting foundational data are troubling.
At present, our conclusion is that there is no evidence that children under eighteen need to be vaccinated. The data doesn’t support it. Like all infectious diseases, we should monitor changes in the data and change directions if we need to.
Introduction
Even after Jenner developed the first vaccine for smallpox, opposition arose quickly as the 1802 cartoon parody shows. The effectiveness and success of smallpox vaccine which eliminated a scourge of perhaps 500 million deaths has long been forgotten even though the disease was declared eradicated only four decades ago. A vaccine’s success always seems to fade away, never to be remembered by naysayers; the old adage “out of sight, out of mind” was never truer. All subsequent vaccines garnered similar criticisms to one degree or another.
Following in the footsteps of the smallpox vaccine, similarly recent improvements in the whooping cough vaccine have been forgotten. In 1986 as I began pediatric practice, about four to six children a month experienced fever in the 104°F range because of whole-cell pertussis vaccine. Despite studies that showed these children were not harmed, this was ammunition for vaccine critics. The acellular pertussis vaccine replaced it and the frequency of these high fevers decreased to between four to six children over two to three years. The success of the improved vaccine once again worked against vaccination efforts. When it was later shown that a three-week cough in an adult correlated with a pertussis diagnosis, even educated parents seemed to shrug off the vaccine’s importance. Once again, out of sight meant out of mind.
The coronavirus vaccine is now here, and opposition has whipped up a political and pseudo-scientific dust devil like never before. The furor over vaccinating children for it far exceeds that in adults. Maurice Hilleman’s flu vaccine prevented the flu epidemic of 1957,1 but who remembers this today. It is just as likely that public sentiments with the coronavirus vaccination will fade into the same apathy about influenza vaccination once this pandemic is behind us.
Two key issues with the coronavirus vaccine force greater scrutiny than previous vaccines, even more so that the very first smallpox vaccine. First, the general public and many physicians are unaware of mRNA vaccine technology, even though it has been around for about twenty-five years. Second, when the new vaccine technology produced the SARS-CoV-2 vaccine so much more quickly than all previous vaccines, it ignited even greater public distrust than that of previous vaccines.
Clearly the past sordid history of vaccine manufacture and testing in mentally challenged individuals even as recently as the 1950s played some part in this. However, even most medical professionals do not know of the bioethical lines that were crossed when vaccines were once tested first on mentally disabled at places like Willowbrook State School in Staten Island and Polk State School near Pittsburgh.2 Every vaccine researcher presented their own justifications for those atrocious actions. Today, once this sordid vaccine past is out of sight and out of mind.
Vaccine development cannot be seen as pure as driven white snow. The means do not justify the end, no matter how good the vaccine. Parents absolutely do have the right to refuse vaccination for their children, and no one has the right to shame them. Shaming can be ever so subtle as a billboard that says, “Do your part, wear a mask and vaccinate.” Expulsion from a medical practice is not subtle, but it is still a form of shaming. It reminds me of when I first read George Orwell’s Animal Farm.
Nobody ever convinced a parent to immunize by coercion. Changing minds about vaccines requires factual information and gentle communication with parents. That requires effort. I cannot make any parent’s vaccine decision for them, but I must respect their decision to go against my vaccination recommendations. Physicians must take the high ground for the children’s sake if parental opinions about vaccination are to change.
What we corporately recommend for the coronavirus vaccination in children will shape future public responses for all vaccines. It is imperative to answer certain questions based on sound data rather than emotional knee-jerk. Should we immunize children with this new mRNA vaccine? Is it safe and effective? Is it wise and financially worthwhile? Individually, how should physicians try to educate parents? That last question is a discussion for another time, perhaps.
What Is an mRNA Vaccine Anyway?
In order to answer these questions, we need first to review the history of the first vaccine for smallpox, then we need to understand mRNA vaccines. Edward Jenner and others observed that cowpox infection in milkmaids protected them from smallpox. Had this fortuitous relationship between coxpow and smallpox not existed, we might still have smallpox in the world today.
On May 14, 1796, Jenner inoculated a young boy named James Phipps with infectious cowpox scab material hoping to capitalize on this relationship between cowpox and smallpox. Six weeks later he exposed Phipps to smallpox and found him to be immune to infection. Jenner repeated this some twenty times, proving without a doubt that variolation (exposing an unvaccinated person to pustular material from the pox vesicle of another) was definitively effective. (James Phipps was not named in the specific publication by Jenner, but his sister was variolated as he reported in his second publication.) 3 4
Variolation with cowpox depended on the presence of cows with active vesicular cowpox lesions. When infected cows were not available, the chain of cowpox variolation went from the pustular material of one vaccinated person to the next vaccinee. Jenner, of course, had no inkling of the other possible viral or bacterial agents that he was passing on through chained variolation. No doubt, the lack of a general understanding contagion by using pus material this way protected Jenner somewhat from public scrutiny. The first hepatitis B vaccine made by Maurice Hilleman many years later which used serum from infected individuals as the vaccine raised many eyebrows. Even those who helped him develop the vaccine were afraid to take Hilleman “purified” human extract.5
The rabies vaccine subsequently developed by Louis Pasteur moved beyond using Jenner’s viral similarity. He dried strips of spinal cords from rabies-infected rabbits to induce immunity using the killed rabies virus itself. Strips of spinal cord from infected rabbits were dried for fifteen days before being ground up and injected into laboratory animals. It uniformly failed to cause rabies, and he found it protected these animals from later exposure to the virus.
On July 4, 1885, a nine-year-old boy named Joseph Meister was bitten at least a dozen times on his hands and arms by a rabid dog. Two days after the attack, his mother brought him to Pasteur’s laboratory, begging him to save her son from the certain death of rabies. Pasteur had never tried his method on humans. Faced with a compassionate need, he injected Joseph first with 15-day-old dried and ground up spinal cord. Every day Pasteur injected the boy with spinal cord dried for one day less than before until on July 16, when he received his final one-day-old dried spinal cord dose. It worked, and the public hailed Pasteur as a hero. Joseph Meister, who held him in great esteem, lived until age sixty when he committed suicide after the Nazi’s forced him to open Louis Pasteur’s tomb. 6
Neither Jenner nor Pasteur understood what caused smallpox or rabies. It wasn’t until 1898 that Martinus Beijerinck proved viral particles even existed. He found that porcelain filters prevented bacteria from passing through, while viral particles penetrated easily.7 He concluded that viruses, unlike bacteria, required intracellular biochemical machinery in order to reproduce. For this work, Martinus Beijerinck is known as the father of virology.
Years of viral research ensued, and our understanding increased vastly. Viruses, of course, cannot reproduce themselves independently of a living host cell. Beyond the DNA or RNA protein map strands enclosed within a lipid and protein envelope, they bear no other resemblance to truly living host cells and are unaffected by antibiotics. Antiviral agents can only affect the few enzyme proteins that viruses require to replicate themselves. Besides the enzyme proteins within the viral particle, or capsid, there are proteins in the viral lipid coat, most recently called spike proteins. Spike proteins act like sticky tape between the virus and the host cell.
These viral enzyme proteins hijack the host cell’s protein producing machinery comprising ribosomes, mRNA, and tRNA. Once viral particles fill the host cell, they are released to infect other cells in a cascading fashion. The organism’s main defense is to produce antibodies. These protein antibodies have the ability to stick to and cover the viral lipid proteins, and so prevent attachment and halt host cell infection.
Jenner and Pasteur both saw the creation of antibodies in response to a whole virus particle. Not only can there be many different proteins in a viral lipid coat, these proteins can change, especially when the reproduction cascades through a single species many times. Cowpox was good at infecting cows, but not quite as good at infecting humans. Influenza started in birds, then jumped to pigs, and then finally to humans. Ebolavirus Zaire, the most serious Ebolavirus strain, looks very much like Ebolavirus Reston which decimates monkeys but not humans. Once a virus transfers to a different species, multiple serial infections within that species cause it to adapt for that species. Thus, as it adapts to new species, it loses some infectivity to old species. We call this attenuation and it is a prime method of producing vaccines.
All viruses mutate, especially when they cross species and attenuate. By that we mean they change the proteins in the lipid coat as infection cascades within one species and also between species. From time to time we get more serious strains of influenza for that reason. Symmetrel was once a good antiviral agent until the flu mutated. Tamiflu supplanted it, but it is surely only a matter of time before it too fails.
We cannot produce enough antivirals or antibacterials to combat infectious agents. The only real treatment is prevention. By that I mean, the only way we can really stay up with the mutations is to assist our built-in immune system. It is not the vaccine itself that kills the virus. It is the host antibodies that the immune system produces which do the work.
Maurice Hilleman’s first hepatitis B “vaccine” may really be where the idea for mRNA vaccines probably started. Hepatitis B produces massive quantities of its spike protein, which is not incorporated into the viral capsid lipid coat but floats free in the bloodstream. This free-floating spike protein swarm attaches itself to hepatitis B antibodies thus shielding the hepatitis viral particle itself which escapes to continue further infection. Maurice’s vaccine came from the filtered serum of infected individuals which was a purified and concentrated dose of only the spike proteins. Filtration, hopefully, removed all the hepatitis B virus itself. Giving only the spike proteins allows the host’s immune system to learn and create antibodies which will already be present and prevent the hepatitis B reproduction cascade in the first place.
The problem with Hilleman’s vaccine was the question of purity. If only one hepatitis B virus got through the filtration, then infection could ensue. Fresh on everyone’s mind was the Cutter Incident where thousands of children were injected with polio vaccine containing live polio virus due to filter failure.8
Could we produce these spike proteins safely and without any possibility of live virus contamination?
In the 1990s, Katalin Karikó started working with the idea that we could utilize the host cell’s protein factory to create only these viral spike proteins. mRNA is a short string of nucleic acid triplets created from the host cell DNA map, and they produce only one protein. tRNA is also a short string of nucleic acid triplets which attach to specific amino acids from which proteins are made. The ribosome, itself a protein, reads the mRNA like a ticker tape one triplet at a time. Each triplet matches with its specific tRNA. With its specific amino acid in tow, the ribosome matches the mRNA and tRNA triplets and then links the tRNA amino acid in an ever-growing protein chain.
At the time Karikó was working on mRNA vaccines, the vaccine industry was still focused on non-mRNA vaccine technologies. These technologies centered around injecting live, but relatively innocuous versions of live virus or dead parts of bacteria. This exposed the host immune system to a multitude of proteins on and within their lipid coats. Some vaccines worked well, but others were problematic.
In particular, pertussis (whooping cough) vaccine was first given as a “whole cell” vaccine. This multitude of pertussis proteins caused the high fevers and other frequent side effects. The acellular pertussis vaccine supplanted it and secondary reactions abated dramatically. In my experience, the frequency of four to six children a month with fever of 104°F or higher decreased to that same number over three years! This vaccine milestone reduced pertussis infection dramatically. The vaccine was better because it was more targeted to produce antibodies against key infectious proteins.
Targeting the right infectious proteins will be the focus of all future vaccines, no doubt. The rapid decoding of DNA genomes of viruses allow us to quickly pick the right target protein. Because mRNA vaccines do not require living host cells for production, they can be mass produced much faster. To date, the fastest vaccine development from start to finish was four years for mumps vaccine.
Current mRNA Vaccines
Contrary to what many think, SARS-CoV-2 vaccine is not the first mRNA vaccine. The first mRNA vaccine was for Ebolavirus Zaire, and it used a virus vector called the Vesicular Stomatitis Virus (VSV), an RNA virus, indirectly carries the mRNA into the host cell. The virus vector has the spike protein RNA genetic code replaced with that of the Ebolavirus spike protein RNA.9 Once the virus is inside the host cell, the mRNA that is produced from that gene causes production of the Ebolavirus spike protein instead. The VSV vector is essential since any mRNA injected by itself would be destroyed almost immediately. The mRNA would never get inside the host cell to produce the target protein the immune system needs to see. The WHO approved the ERVEBO vaccine for emergency use in Africa in 2018, and it was FDA approved in 2019. ERVEBO was very effective in stopping urban Ebola in Africa, proving the value of mRNA vaccine technology.
Lipid coat technology used in the SARS-CoV-2 vaccine negated the need for any viral vector. The lipid coating protects the mRNA until the host cell absorbs it just like a virus. Viral contaminants like SV40 have always concerned early vaccine pioneers, but are not a problem with lipid-coated mRNA vaccines.
Each company that developed a SARS-CoV-2 vaccine creates its own mRNA using the complete genome of the virus. Genomic mapping is quick. The entire SARS-CoV-2 genome was known within a couple of days. Geneticists can now quickly determine which segments map to the specific mRNA for the viral spike protein. Manufacture can begin quickly, while it is the vaccine trials phases that take the most time now.
The Future of mRNA Vaccines
The future of mRNA vaccines looks bright. Likely we will see most future vaccines developed precisely like the current SARS-CoV-2 mRNA vaccine. It also seems likely that older vaccines would be revisited to see if the mRNA technology could benefit them.
A primary contention with vaccine manufacture has been the use of fetal cell strains, such as WI-38 for production. Past vaccine manufacture relied on a supply of target virus, and viruses only grow living cells. Use of monkeys and other species had been proven to introduce other viruses into the vaccine such as SV40. Fertilized chicken eggs are a favored growth medium, since the membrane lining next to the shell grows some target viruses like measles very well. When the SV40 monkey virus was discovered, the FDA would only allow the use of human cells in vaccine manufacture. The cells must be normal human cells.
Cell strains are developed from teasing live human cells out of tissue onto plates. Unlike human cancer cells, such as the HELA cell line, cell strains are not immortal. The ethical objections to creating cell strains from fetal cells should be obvious. However, while no fetal cells are used or included in the vaccine injections, the sad story of the history of WI-3810 moves people to be concerned that unborn children would be aborted specifically to harvest cells for new cell strains. These are genuine concerns, but opponents to vaccination are often keen to distort the truth, essentially saying that tomorrow’s vaccines contain material from today’s aborted babies. That is factually false.
At the time Hilleman was developing the vaccine, chickens were widely infected with the chicken leukemia virus. He would not consider using the eggs of any infected chickens for fear that the chicken leukemia virus might be injected with the target virus vaccine. No one then knew if chicken leukemia virus could cause cancer in humans.
Because mRNA vaccines contain no complete virus DNA or RNA, they can never infect a vaccinee. Cell strains have a limited number of replications. We are almost at the end of the WI-38 cell strain. mRNA vaccines could remove reliance on cell strains once and for all. It is fairly hard to find a concise list of vaccines that currently use cell strains for production, but here are ones I’ve seen reported on a web search.
- Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
- Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
- Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
- Zoster (shingles) vaccine [Zostavax/Merck]
- Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] – not given routinely
- Rabies vaccine [IMOVAX/Sanofi Pasteur] – not given routinely
The only gold found in the coronavirus pandemic has been a practical demonstration that lipid-coated mRNA vaccines can be made much more quickly, and without the concerns of past vaccines for viral contamination or the need for viral vectors to get mRNA into the cells, among other historical contentions. Past vaccine development compared to current vaccine development is like comparing battlefield mortar shelling to cruise missiles. The SARS-CoV-2 pandemic changed future vaccine development almost overnight.
Should Children Get the SARS-CoV-2 Vaccine?
Everything presented above lays the foundation for this question which is actually not one question. It comprises multiple questions.
What are the driving forces for vaccination and how accurate is testing?
Before the SARS-CoV-2 pandemic ever landed on US soil, I was watching closely. I began following the numbers in multiple countries and tried to teach my patients through well-thought-out posts on Facebook as fear became palpable everywhere. I created detailed spreadsheets following case numbers day by day in the US and a number of other countries. I graphed this data daily and posted my assessment state by state and country by country. Positive cases continued to increase as expected in viral exponential growth. I shared the video “Exponential Growth and Epidemics” by 3Blue1Brown,11 and I explained to those following me that what we were looking for was the inflection point in that curve. That would indicate the growth of cases and the pandemic was on the way out. I described how each geographic area of the world would reach inflection at different times.
Shortly after that PCR (Polymerase Chain Reaction) analysis for the virus became available, testing required a physician’s order. A discussion via phone or face-to-face office visit between patient and provider demonstrating the required presence of symptoms was absolutely necessary then. Testing capacity ramped up as cases increased.
Then something changed. Patients no longer had to get a physician order to be tested. I began to hear patients and friends tell me they wanted to get tested because they thought they might have had the virus even before the first confirmed cases in the US. Not understanding PCR testing, the public suddenly had a hydra on its hands. Fear increased and led to lockdowns, mask mandates, and shaming of those opposing masks by those wearing them. Testing took on a life of its own complete with its profitable nature.
Soon (as I write this), I fly to Amsterdam and on to Tanzania to be a part of a medical mission work deep in the bush. Schiphol airport requires specific PCR testing be done 72 hours before arrival even for passengers with results in hand to verify a negative test. I chose to get vaccinated in order to reduce the possibility of a positive test. I have never been symptomatic, but some people are testing positive weeks after symptoms are gone or even after they have been vaccinated.
Is it possible that positive PCR testing can be faulty? Are positives after immunization simply vaccinations that fail to take?
The PCR tests have proven to show different results based on the cycle threshold. Polymerase acts on nucleic acid strings to make multiple copies to amplify the presence of either a complete, or even partial segment of, viral RNA or DNA. Repeated exposure to polymerase over and over amplifies the number of viral RNA or DNA exponentially. The number of repetitions before the testing of the presence of specific RNA or DNA is called the Ct, or cycle threshold.
Oddly, the cycle threshold for SARS-CoV-2 testing varies from country to country. Even worse, the CDC has curiously adjusted the recommended Ct down with one high profile expert reporting that high cycles represented “dead nucleotides.”12 What are dead nucleotides? For this pandemic, these are fragments of destroyed SARS-CoV-2 virus. This brings up the question about what any positive PCR positive test means without confirmatory testing by other methods and a history of symptoms.
What began as good science and good medicine has become a detriment. The public generally thinks that a positive PCR absolutely means SARS-CoV-2 infection. This is patently false. Somehow PCR testing went from being a screening test to a definitive diagnosis.
What do these dead nucleotides indicate if someone has been asymptomatic for SARS-CoV-2? There are two kinds of immunity: innate and acquired. Acquired immunity results from exposure to infectious agents or vaccines which mimic them. Innate immunity is present without any exposure to an infectious agent or vaccine and it is not well understood. In 1984, Stephen Crohn became known as the man who couldn’t catch HIV (Human Immunodeficiency Virus). Despite repeated sexual exposure to HIV infected partners, he never caught the virus. He had a genetic mutation which provided him with an innate immunity.
I suspect innate immunity to the SARS-CoV-2 virus may well be why we see dead nucleotides in asymptomatic people who have positive PCR tests. They defeat the virus which never actually infects their cells, and the dead nucleotide fragments end up on their mucous membranes. Perhaps we will confirm this just as it was confirmed in Stephen Crohn.
In the American Institute for Economic Research, an article13 by Paul E Alexander MSc PhD, Howard C. Tenenbaum DDS, and Parvez Dara, MD cite some interesting primary data pertinent to SARS-CoV-2 illness and asymptomatic positive PCR tests. In particular a French study14 concluded that in an asymptomatic child with an RT-PCR positive test, there was no evidence the child transmitted SARS-CoV-2 to any of the three schools they visited. Is this a case-in-point for innate immunity and/or faulty PCR testing?
They also cite this study15 which demonstrated no transmission of disease from asymptomatic PCR positives in Wuhan, China where the pandemic started. Dr. Maria Van Kerkhove of the WHO echos this in this video.16 This further improves the idea that there must be other reasons beside host cell infection for asymptomatic positives.
Alexander and his colleagues also cite an article from the New England Journal of Medicine.17 In March, 2020, early in the pandemic, Sweden decided to keep their schools open unlike many other countries. The number of deaths in 2019 prior to the pandemic were 65 of the 1,951,905 Swedish children. From March through June 2020 during prime pandemic, they saw 15 children with SARS-CoV-2 admitted to the ICU, some with MIS-C (Multiple Inflammatory Syndrome Coronavirus). None of them died. How they were diagnosed is not clear from the article.
At some point, politics preempted science. Stricter policies in various states have failed to show any consistent effectiveness, and some states with the more draconian mandates have had higher testing numbers. The success or failures in a state have largely been judged by the numbers of positive PCR tests. The success or failures in a state have largely been judged by the numbers of positive PCR tests. Proponents of universal vaccination base their recommendations on PCR positives which are not indicative of true cases, and this calls into question their motives. The change in CMS (Centers for Medicaid and Medicare Services) changed diagnosis coding in hospitals and increased remuneration for those patients with a primary SARS-CoV-2 diagnosis. The hydra became a kraken. In a CDC report, now removed I think from their website, they admitted that only 6% of the 400,000 to 500,000 SARS-CoV-2 deaths were strictly from the virus. All the other individuals had medical conditions which were life-threatening, and prone to die from any number of mitigating illnesses that would push them over the cliff.
Who’s data can we trust now? I’m not sure, but PCR positive numbers are meaningless to make public policy. I’m deeply concerned about the way medicine has lost control here. Within this cloud of confusion, now the recommendation is to vaccinate children all the way down to six months. I fear that policy will trump good medicine.
Is an mRNA vaccine safe for use in children?
The closest past evidence of safety was used under the WHO compassionate clinical protocol of the ERVEBO viral vector mRNA Ebolavirus vaccine in the Ituri, North Kivu, and South Kivu districts of the Democratic Republic of Congo in the 2018-2020 EBOV outbreak. The usual limitation to non-pregnant, non-lactating females and all males 18 and over was extended down to six months for all individuals per the recommendation of the Strategic Advisory Group of Experts (SAGE).18 A full review of the safety data is expected in early 2021, but preliminary reports.
While the vaccine was 100% effective, according to the WHO, people were still cautioned. Ebolavirus is a Biosafety Level 4 agent, and all body fluids teem with virus.18
In March 2021, Pfizer and Moderna started global Phase 1, 2, and 3 safety and efficacy pediatric trials with their mRNA SARS-CoV-2 vaccines for ages six months to eleven years with high hopes after promising results in 12 to 17-year-olds that began in July 2020.20 21
Some have suggested that the mRNA lipid nanoparticles in the SARS-CoV-2 nanoparticles are dangerous. That is unclear at this point, and needs to be studied. Given the past history of vaccine development laid out above, the mRNA in the vaccines appears not only to be safe, but easily and quickly improved as needed for future viral mutations.
Is the vaccine helpful for SARS-CoV-2, i.e., does the mRNA coronavirus vaccine work?
This question is important beyond safety and efficacy vaccine trials. It aims straight for the political controversy of mass mandatory vaccination.
Consider the history of yellow fever. No one in the U.S. today vaccinates routinely for it. Yet, in the 18th century it rampaged across colonial America and West Africa, but by the end of World War II we eradicated in the U.S. through vaccination and mosquito control.22 Today, vaccination for U.S. citizens is indicated for those traveling to countries where yellow fever is still a present threat. We don’t use the vaccine on everyone just because we have it.
In 2009, when the same H1N1 strain of influenza (the infamous Spanish flu) burst back on the scene, there were specific patient age groups who were more affected. Recall that killed 25 to 50 million of the world’s then. I was born in 1958 when H1N1 was still going around some, though between pandemics, and I likely had some immunologic experience as did others my age. The most affected age groups I saw in my office in 2009 were adolescents and pregnant women, not those in older age groups or younger children.
Conclusion
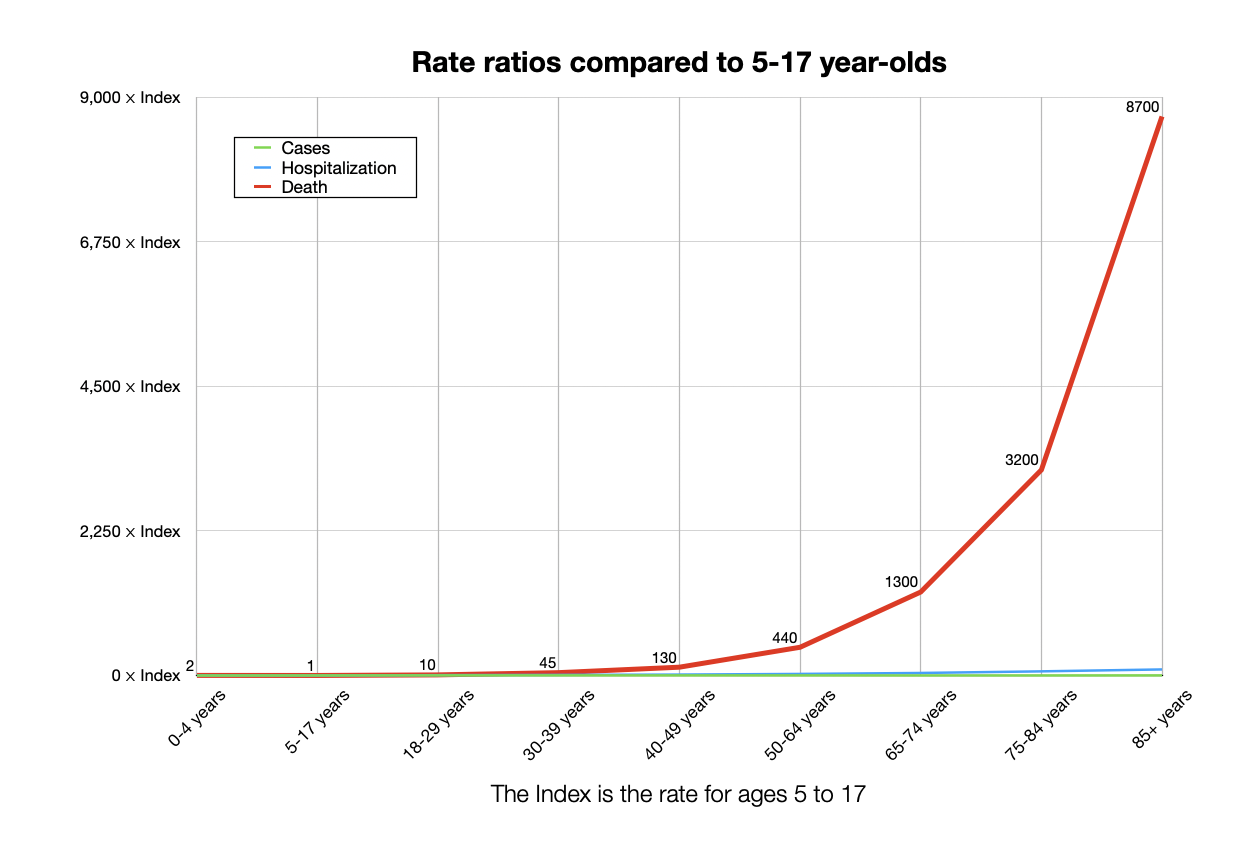
Similar assessment of the need and benefit of SARS-CoV-2 vaccine is critical. More safety data needs to be accumulated. The graph below is from the CDC and was updated on February 18, 2021.23 The numbers shown are risk ratios of all ages compared to ages 15 to 17 years. What this shows is how low-risk younger children and adolescents are compared to those of increasing age. Race and ethnicity don’t seem to vary enough to make any difference from the CDC data.24
What is clear from this graph is that the ratios of cases, hospitalizations, and deaths are very low in all pediatric ages. Absolute incidence of pediatric cases continues to be very low warranting CDC recommendations to go back to in-school learning. While the vaccine safety and efficacy is important and yet to be established, these data together do not support routine or mandatory emergency pediatric vaccination since it would make no difference to disease occurrence in children or adults. We have time to gather more data. We should wait therefore before vaccinating children under the age of 18 with the SARS-CoV-2 mRNA vaccine.
Bibliography
ENDNOTES
- Offit, Vaccinated, p. 12-17 ↩
- Offit, Vaccinated, p. 21-28 ↩
- Offit, Vaccinated, p. 32 ↩
- Jenner, The Three Original Publications On Vaccination Against Smallpox, p. 164-165. ↩
- Offit, Vaccinated, p. 117-128. ↩
- Offit, Vaccinated, p. 34-36. ↩
- Beijerinck MW. On a Contagium vivum fluidum causing the Spotdisease of the Tobacco-leaves. Koninklijke Nederlandse Akademie van Wetenschappen. 1898;65(2):3-21. ↩
- Offit PA. The Cutter incident, 50 years later. NEJM. 2005;352(14):1411-1412. https://www.nejm.org/doi/pdf/10.1056/NEJMp048180 ↩
- Domachowske, Vaccines: A Clinical Overview and Practical Guide. p. 147 ↩
- Leiva, A Brief History of Human Diploid Cell Strains. The National Catholic Bioethics Quarterly. 2006;6(3):443-451. ↩
- https://www.youtube.com/watch?v=Kas0tIxDvrg ↩
- https://principia-scientific.com/dr-fauci-admits-covid-test-picks-up-harmless-dead-virus/ ↩
- https://www.aier.org/article/why-we-must-not-be-forced-into-vaccinating-our-children-from-covid-beware/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7184384/ ↩
- https://www.nature.com/articles/s41467-020-19802-w ↩
- https://www.youtube.com/watch?v=NQTBlbx1Xjs ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7821981/ ↩
- https://www.who.int/news-room/q-a-detail/ebola-vaccines ↩
- https://www.who.int/news-room/q-a-detail/ebola-vaccines ↩
- https://www.pfizer.com/science/clinical-trials/children ↩
- https://www.webmd.com/vaccines/covid-19-vaccine/news/20210316/moderna-launches-clinical-trials-on-young-children ↩
- Plotkin, Plotkin’s Vaccines, p. 1181 ↩
- https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html ↩
- https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html ↩
 Copyright secured by Digiprove © 2021 Ronnie Smith
Copyright secured by Digiprove © 2021 Ronnie Smith